Thailand
- Background
Although stronger tobacco control policies were developed and implemented in early 1990s, the health budget for health promotion and tobacco control was not only limited but also showed a decreasing trend. This led to a movement to secure more stable, regular, sustainable funding for health promotion. A health promotion fund was proposed simultaneously with the idea of setting up a universal health insurance fund, and a study on a health financing model from a dedicated excise tax under the control of an autonomous agency established by the State was initiated. After eight years (1993–2001) of planning, strategy and cooperation among the stakeholders and partners, and with strong support from the tobacco control movement, the Thailand Health Promotion Foundation (ThaiHealth) was formed in 2001 and enacted as an independent organization under the Health Promotion Foundation Act (BE 2544)[1].
- Process that led to adoption of the Health Promotion Foundation Act
The movement to find innovative funding for health promotion was initiated by two dedicated health advocates, Dr Prakit Vathesatogkit and Dr Supakorn Buasaiin late 1995. The Fiscal and Financial Master Plan (1997–2001) of the Ministry of Finance included proposals for both a health insurance scheme and a health promotion fund. These were accepted with the proviso that a fund should also be established to promote health in the general public and another to provide medical welfare in line with the concept of fiscal and financial policy for social development promoted by the Ministry of Finance. To support the proposals, a working group was set up to establish a private or public health promotion institute and a health promotion and a health insurance scheme or fund on 9 August 1996.
The health promotion movement was supported by various ministries, including those of Finance and Public Health, Government organizations (the Health System Research Institute), NGOs (e.g. Action on Smoking and Health Foundation), academia, WHO, health professionals and the public. Advocates used various strategies to convince policy-makers and to mobilize support from diverse groups for a health promotion foundation with sustainable funding. The activities included organizing a series of scientific conferences and meetings, consultations, public fora with various stakeholders and participating in regional and international conferences on health promotion. Study tours with leading advocates for health promotion were important for gaining the support of high-ranking policy-makers at the ministries of Finance and Public Health, the Finance and Fiscal Bureau and the Health System Research Institute. A study tour was also organized to the Victorian Health Promotion Foundation, Australia, and the Health Sponsorship Council, New Zealand, to learn about organizational structure, operations, problems, limitations and sources of revenue, particularly the use of “sin taxes” for health promotion. Another strategy was to ask experts from the Victorian Health Promotion Foundation to share their experience and to make a courtesy call to the Minister of Finance and other policy-makers for discussions on health promotion.
The Health System Research Institute compiled and synthesized local and international evidence for advocacy messages for the health promotion foundation. It also supported and undertook joint research among researchers, academics and leading advocates on the fiscal and health impacts of a tax increase, price elasticity and demand analysis, health care costs, the health impact of smoking, a desk review of foreign legislation on health promotion funds, a health financing model from dedicated excise tax, a benefit–cost analysis of establishing a Thai health promotion foundation, the evolution of tobacco consumption control, a public poll to support use of “surcharge sin taxes” for health promotion and lessons learnt and experience from other health promotion foundations.
The initial bill proposed to establish the ThaiHealth Office funded by a dedicated tax was not endorsed by the Ministry of Finance, which objected to an earmarked tax. At the same time, however, a bill on a Campaign Fund for Cessation of Alcohol and Tobacco Consumption was proposed by the Excise Department, which authorized the Ministry of Finance to collect revenue from producers and importers of alcohol beverages and tobacco. The bill was drafted after the Cabinet liberalized the alcohol trade. Concern was raised about the impact of such policy and whether a mechanism was required to reduce alcohol consumption by imposing an alcohol tax. The Deputy Minister of Finance proposed that the two bills be combined into one ThaiHealth bill, which had a clear organizational structure, function and management with the source of funding yet to be decided, while the other bill has a funding source but lacked operational details.
In the early years of advocacy (1995–1998), it was suggested that the new health promotion agency receive approximately 1% of the public health budget annually, corresponding to about 700 million baht (USD 19.5 million), representing about 2.5% of the cigarette excise tax at that time. This was based on the premise that the Government would invest 1% of the Ministry of Health budget for health promotion. In 1999, when the Deputy Finance Minister expressed support for the combined bill, the proposed budget was 2 billion (USD 0.06 billion) rather than 700 million baht, on the premise that ThaiHealth should receive the same amount as the AIDS unit of the Ministry of Public Health, as it covered more health promotion issues than AIDS. In addition, the estimated economic loss due to tobacco and alcohol consumption and traffic accidents was a further 200 billion baht (USD 5.58 billion) annually. If 2 billion baht were invested in health promotion and reduced the problem by 10%, 10% of economic losses would be saved, resulting in about 20 billion baht (USD 0.56 billion) total loss. The proposed 2 billion baht budget for the new agency is equivalent to 2% of the surcharge taxes on tobacco and alcohol; therefore, that rate has been used for advocacy.
During advocacy for a 2% surcharge tax for health promotion, strong challenges were raise, particularly from the Ministry of Finance, which raised concern about the cost–effectiveness of the investment and the legitimacy of using tax revenues from alcohol and tobacco to sup- port programmes and activities that are unrelated to these products. They also argued that the funds from the tax would be misused for other purposes or result in corruption and that a surcharge tax would set a precedent and may disrupt the country’s “financial discipline” if replicated. The Deputy Minister of Finance requested an official search to determine whether any law prohibited a surcharge tax. As none was found, the proposal for a surcharge tax was presented for consideration by Parliament as a useful investment for the country.
The Ministry of Public Health proposed that the health promotion foundation be placed under its jurisdiction but was concerned that it might duplicate its Division of Health Promotion. Those concerns were addressed by evidence from local and international studies and the positive experience of other health promotion foundations that a health promotion programme under a Ministry of Health is service based, while the new health promotion agency would conduct population-based activities. Frequent changes in Government leadership, Cabinet ministers and Government officials meant that the proposals stalled for a while and were reviewed intermittently. It is interesting to note that there was less resistance from the tobacco industry on the proposal to use the surcharge tax for the ThaiHealth Foundation, as it replaced the proposal for a tobacco tax increase; this also helped to dampen opposition from the Ministry of Finance, as the tobacco industry would pay more on tax if the tobacco tax increased by more than the 2% surcharge tax. Another argument was that the main reason for setting up a health promotion fund was to improve health in various areas. There was poor understanding of the overall objectives and actual work of ThaiHealth.
The draft Royal Decree for establishment of the Thai health promotion agency under the Public Organization Act 1999 was approved by the Thai Cabinet on 19 October 1999 and made into law by His Majesty the King on 30 June 2000. Simultaneously, a bill to set up a dedicated fund for cigarette and alcohol taxes as a regular, sustainable source of revenue for the agency was proposed. It was approved by Parliament on 26 September 2001 and came into force on 8 November 2001. This gave birth to the ThaiHealth Foundation with a 2% dedicated surcharge tax on tobacco and alcohol. In all, it took about 2 years from the time the bill was submitted to Parliament to adoption of the Health Promotion Foundation Act in 2001.
The ThaiHealth office was first operated under Public Organization Act BE 2542 (1999), while awaiting the coming into force of legislative processes for the health promotion bill based on surcharge taxes. An estimated 150 million baht were allocated for ThaiHealth’s first year of operation, but only a fraction was spent, as the ThaiHealth office was busy drafting the funding mechanism and other regulations in the early stages of its establishment.
It took about 7 years (1995–2001) of consolidated effort to get the adoption of the Act, due to the work of highly committed and determined individuals who are respected for their integrity and hold prominent positions in society, with access to key policy-makers. Continuous sup- port from other advocates, civil society and policy allies at various stages of the process also
helped to overcome obstacles. The Health System Research Institute played a significant role in knowledge management, including compiling, generating, synthesizing and disseminating resources for policy advocacy, knowledge transfer and awareness-raising among policy-makers and the general public. The main principle of the surcharge tax is that tobacco and alcohol producers pay an additional 2% excise tax for the health promotion foundation as a new funding mechanism that is not restricted by financial or other legislation in Thailand.
- The ThaiHealth Promotion Foundation
The Health Promotion Foundation Act (BE 2544)[2] legally founded ThaiHealth as an autonomous State agency outside the formal structures of Government. Thus, ThaiHealth is not man- aged by the bureaucratic system of the Ministry of Public Health and is under the supervision of the Prime Minister. As an autonomous agency, ThaiHealth can work with various ministries and with agencies in both the public and private sectors. It is therefore not bogged down by bureaucratic processes and is free of interference from ministers and ministry officials.
ThaiHealth has two governing arms: the multi-sector Board of Governance and the Evaluation Board. The Board of Governance comprises 21 members. It is chaired by the Prime Minister; the Minister of Public Health is the first Vice-Chairman, and an independent expert appointed by the Cabinet is the second Vice-Chairman. Of the remaining Board members, nine are representatives from ministries and another eight are independent experts in various disciplines who have no political affiliation but are chosen as qualified honorary members from the com- munity. The Board sets policies, regulations, strategies and the overall budget and oversees the management and other guidelines for ThaiHealth. The Board takes also advice from a series of expert advisory committees. The Evaluation Board has seven members, who are experts in health promotion, finance and evaluation, and are responsible for evaluating the overall performance in policy-making, activities and operations, in order to ensure accountability, transparency and efficiency. The two boards, which are appointed by the Executive Cabinet, have equal standing. ThaiHealth is guided by a Chief Executive Officer, who is a member of the Board and also act as the secretary[3],[4],[5].
3.1 Funding mechanism and management[6]
The Act entitled ThaiHealth to collect a 2% surcharge on the tax levied on alcohol and tobacco. Thus, tobacco and alcohol producers are required to pay an additional tax on top of the excise tax, which is dedication to the health promotion fund. This type of legislated funding mechanism may be the most effective means for securing sustainable long-term funding for health promotion, because tobacco and alcohol taxes are a highly predictable, reliable source of revenue. The mechanism provides sustainable funding by a Parliamentary Act, which safeguards the fund from easy abolishment by the industry. As the surcharge tax is used to support health promotion projects to improve public well-being, a politician or Government official who plans to abolish the fund will not be respected by the public.
In practice, the Excise and Customs departments are responsible for invoicing the levy, which is remitted directly to the Foundation without going through the Ministry of Finance. The dedicated revenue is thus transferred directly to the ThaiHealth bank account (at Krung Thai Bank PCL) and is administered by the financial and accounting unit. The fund is not subjected to normal budgetary processes.
The Governance Board has the power and duty to control the transparency and accountability of the fund flow and distribution and to supervise the operation of the foundation. A finance sub-committee assists in managing and supervising financial issues. Generally, ThaiHealth is governed by an independent board and is audited by a designated Government agency, the Auditor General of Thailand. It is required to submit a report on performance and a financial summary annually to the Cabinet and to both houses of Parliament (the House of Representatives and the Senate). It is supported by a number of expert advisory committees. At project level, all ThaiHealth’s grantees are subjected to financial and accounting audits by a certified public accountant.
Funds are allocated for proactive and open grants, with some allocation for unplanned or emerging health promotion issues, such as adolescent pregnancy. Such projects must obtain approval for funding from the ThaiHealth Governance Board, chaired by the Prime Minister. In 2014, the ThaiHealth annual investment in promoting health was 4 064.74 million baht (USD 125.15 million), equivalent to 1.8% of the combined budget of the Ministry of Public Health and the National Health Security Fund combined[7],[8].
3.2 Collection and distribution of the ThaiHealth fund
Since establishment of the ThaiHealth Foundation in late 2001 (fiscal year 2002), the funding generated from the 2% surcharge tax on tobacco and alcohol has increased steadily as a result of increases in the taxes on tobacco and alcohol products each year. The annual revenue increased from 1.92 billion baht (USD 0.06 billion) in 2003 to 4.06 billion baht (USD 0.14 billion) in 2014. The tax increases are made mainly with the intention of collecting more revenue to fill the Government’s treasury. ThaiHealth’s relentless campaigns to de-normalize tobacco and alcohol products have raised public awareness, so that there has been less public outcry over the tax increases, despite strong opposition from the tobacco and alcohol industries.
ThaiHealth funds projects to address health risks, such as from tobacco and alcohol use, traffic accidents and inadequate physical activity, including research, community programmes, advocacy and mass media campaigns. The Ministry of Public Health does not receive a budget for these activities. The ThaiHealth fund is distributed in 14 plans, covering tobacco and alcohol control, health promotion in communities, social marketing and system support. A healthy community strengthening plan and a plan for a healthy media system and promotion of a spiritual health pathway were given highest the budget allocations of 683.71 million baht (14.5%) and 672.84 million Baht (14.3%), respectively, although the actual disbursement was only 11% and 11.7% of the estimated budget, respectively. The total budget allocation for prevention programmes on the three major health risk factors increased from 264.7 to 308.9 million baht (5.6% to 6.7%) for tobacco control, from 272.7 to 369.6 million baht (5.8% to 8.1%) for alcohol and substance abuse control and from 189.4 to 262.7 million baht (4% to 5.7%) for road safety and disaster management. Similar trends were seen for promotion of healthy children, young people and families, which increased from 261.3 to 280.7 million baht (5.6% to 6.1%), promotion of healthy food, from 169.9 to 262.9 million baht (3.6% to 5.7%), and a health learning centre, from 118 to 154.6 million Baht (2.5% to 3.4%). The total budget distribution for innovative health promotion and open grants rose from 241.3 to 311.5 million baht (5.1% to 6.8%).
The health promotion work of ThaiHealth does not duplicate that of the Ministry of Public Health. The ThaiHealth programmes are population-based and conducted mainly in collaboration with the non-health sector and NGOs, while the programmes and activities of the ministry are provided nationwide at health service centres by various agencies. They include health education, counselling, vaccination, rehabilitation and health education, with some campaigns on a healthy diet and exercise but no mass media campaign due to limited resources. The Ministry of Public Health does not fund project-based programmes and cannot fund NGOs for related health promotion programmes. The budgetary allocations of the ministry and of the health promotion division at the Department of Health are unchanged, and they continue to operate as they did before ThaiHealth was set up. The health promotion division at the ministry received less than 60 million (USD 2 million) baht in 2003, while ThaiHealth’s budget was about 1.9 billion baht (USD 0.06 billion). ThaiHealth funds many Ministry projects that failed to obtain funding from the regular budget and also provides funds to the tobacco and alcohol office. ThaiHealth’s programmes and projects focus on advocacy for the adoption of public health regulations and laws, while the ministry can advocate for policy change only with political approval and may be influenced by groups with vested interests.
ThaiHealth and the ministry collaborate on tobacco and alcohol control, ThaiHealth funding mass media campaigns on physical activity, diet, traffic accidents, research, capacity-building in health promotion and policy advocacy. ThaiHealth also provides funding for health promotion in communities, schools and workplaces.
- Tax implications
ThaiHealth plays a significant role in health beyond that of the ministry by contributing to funding the prevention and control of NCDs. The use of tobacco, alcohol and other harmful substances has decreased over the years. Cigarette excise taxes were increased about 10 times between 1991 and 2011, which resulted in a significant gain in revenue, from 15.898 million baht (USD 530 million) in 1991 to 59.914 million baht (USD 1.997 million) in 2011, and a decreasing trend in smoking prevalence among adults (> 15 years), from 25.47% in 2001 to 20.7% in 2009[9],[10]. Thus, ThaiHealth’s revenue increased with the reduction in smoking prevalence. The “SimSmoke” model[11] shows that, by 2006, tobacco control policies implemented between 1991 and 2006 had already decreased smoking prevalence by 25% as compared with what it would have been in the absence of the policies. Tax increases on cigarettes and advertising bans had the greatest impact, followed by anti-smoking media campaigns, clean air laws and health warnings. It was estimated that the policies saved 31 867 lives by 2006 and will have saved 319456 lives by 2026[11]. A similar reduction rate was reported in alcohol consumption, from 9.1% in 2004 to 7.3% in 2009; the death rate from vehicle accidents decreased from 22.9 per 100 000 in 2003 to 16.82 per 100 000 in 2010. The number of Thai people who exercised regularly increased from 29% in 2003 to 29.6% in 2007[12].
Moreover, the social return of ThaiHealth’s investment in tobacco consumption control (2001– 2010) was 18 times, with a return of 18 baht for every baht spent. This calculation is based on the total direct and indirect cost of 1 433 million baht (USD 47.8 million) and overall outcomes estimated at 189.359 million baht (USD 6 312 million). A higher return, of 130 baht for every baht spent on road traffic accident prevention, is derived from a total expenditure of 1 454 million baht (USD 48.5 million) and an estimated benefit of 26 289 million baht (USD 876.3 million)[13].
ThaiHealth supports a number of national and provincial policies and programmes to pro- mote the well-being of the Thai people. Major legislative changes have been made, such as extension of smoke-free areas in public places, such as open-air markets, restaurants, pubs and bars, increasing the number and size of pictorial health warnings, printing the national quit-line number (1600) on all cigarette packs, banning tobacco advertising at points of sale and prohibiting designations such as “low tar” or “light” on packs. Support for quitting smoking and reducing alcohol consumption was set up in 2008, comprising telephone consultations and therapy, supported by the Government, the private sector and communities. Other developments are an increase in the number of alcohol policies, liability for damage in the Unsafe Product Act, a toy control system, television programme ratings, establishment of an independent public broadcasting television from earmarked tobacco and alcohol excise taxes, prohibiting use of mobile phones while driving without an accessory, a safe, clean Internet cafe policy and prohibition on adding sugar to infant formula. Several institutions have been established to support health promotion programmes, including the Tobacco Control Research and Knowledge Management Centre, the national quit-line, the Quality Learning Foundation and the Social Enterprise Promotion Office. ThaiHealth can support nationwide mass campaigns and community mobilization. Nationwide campaigns have been conducted for the general population and specific groups to introduce a culture of no smoking in public, particularly in urban areas and also in hospitals; 80% of hospitals were smoke-free in 2011.
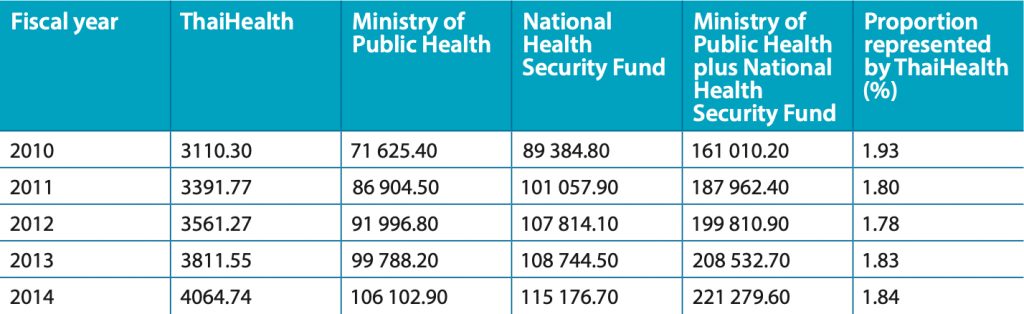
ThaiHealth fund was used mainly for health promotion programs that were not supported by Ministry of Public Health or not within their budget line. ThaiHealth’s role would complement MOPH that focuses on service-oriented curative treatment. Thus, it’s clear that the earmarked revenue for ThaiHealth would not offset any of the national health budgets. Thailand’s national health budget comprises the budgets of the Ministry of Public Health, National Health Security Fund and the health budgets of all other Government agencies, including health care for Government employees and social security for workers, and universities, the military, the police and Bangkok Metropolis Hospital. The annual budget of ThaiHealth represented 1.78–1.84% of that of the Ministry of Public Health and the National Health Security Fund between 2012 and 2014 (Table 1), equivalent to only 1% of the total national health budget. Although the ThaiHealth budget for health promotion is smaller than the total national health budget, it supports many health promotion programmes and activities, which have a significant impact on the health status of Thai people. The funding mechanism itself is a powerful health promotion intervention.
Table 1. Annual budget for health (in million baht), 2010–2014
 Sources: References 6 and 7
Sources: References 6 and 7
4.1 Programme priorities and granting mechanism[14]
In order to prioritize health promotion and disease prevention to ensure a healthy, sustainable environment for Thai society, the plans and strategies of ThaiHealth are aligned with the national health strategy and priorities. ThaiHealth also acts as catalyst to accelerate commitment and implementation of health promotion programmes identified in national policies and plans for health. It also creates and coordinates health promotion in related sectors, mainly through policy advocacy and social mobilization.
Its reliable funding allows ThaiHealth to continue supporting and implementing many short-, medium- and long–term health promotion programmes and innovative projects throughout the country. The fund is distributed to 14 master plans: for issues (tobacco and alcohol control, traffic injuries and disaster management, physical exercise and sports for health, healthy food and diet and control of health risk factors, settings (health of disadvantaged groups, health promotion in the community; child, adolescent and family health and health promotion in organizations; and the health system (social marketing and communication, health promotion in health service systems and a health learning centre. supportive systems and mechanisms and open grants and innovations). The plans being supported have evolved over time, from only seven in 2002. In 2014, about 90% of the budget was spent on these 14 plans and 5% for administrative expenditure; most disbursements (36%) were on activities to decrease the main health risks (tobacco and alcohol consumption, unsafe driving) and increase physical activity and food safety programmes. ThaiHealth has established a broad geographical reach among diverse population groups and sectors for major risk factor reduction programmes.
Implementation of the plans is supported by two types of granting scheme: proactive and open grants. The proactive (strategic) grants are accorded to major health promotion projects initiated by ThaiHealth but implemented by others. ThaiHealth sets the agenda in the framework of the master plan. The grants are based on goal, strategy and partners. An estimated 4 281.79 million Baht (USD 133.8 million) (93.2%) were spent in 2014 on proactive grants. Open or reactive grants are available for any organization and provide opportunities for public participation in health promotion and innovations. These received the remaining 311.49 million baht (USD 9.73 million) or 6.8% of the implementation fund allocation in 2014.
The strategies used to implement the plans include research, awareness and education, social mobilization, capacity-building and policy development for issues, settings, areas and target populations. The approaches and health promotion strategies of ThaiHealth are based on capacity-building, in accordance with the Health Promotion Foundation Act, to foster the capacity and ability to plan, develop and implement health promotion programmes for communities, Government and NGOs, private and public interest organizations, State enterprises and other State agencies.
ThaiHealth supports and complements rather than replacing existing structures and agencies and has extensive strategic partnerships and collaboration with all sectors of society, ranging from national to grassroots networks. Strong partnerships have been formed with diverse population groups, communities, organizations, ministries, Government agencies, private organizations, temples, educational institutions and others. ThaiHealth invested about USD 140 million in 1937 health promoting projects and activities in 2013 and has established networks among 12480 organizations and individuals nationwide more a decade after its inception. The National Health Security Bill, which was proposed simultaneously with the Health Promotion Bill to establish universal health insurance for Thais, was promulgated into law in 2002. It meets the primary goal of providing health security and health promotion.
ThaiHealth encourages interested organizations to apply for open grants for innovative projects and provides stable financial support to long-term projects that meet its objectives. The Foundation also supports programmes for changing public values, lifestyle and the social environment to promote health and well-being. It complements other bodies working in health promotion. It shared its experience and provided mentorship to Mongolia in setting up a health promotion fund, and collaborated with the Southeast Asia Tobacco Control Alliance in mentoring Viet Nam and the Lao People’s Democratic Republic in establishing a tobacco control fund based on a surcharge tax. ThaiHealth is becoming a referral point for study visits and has run several capacity-building workshops to share its experience in using tobacco taxes. ThaiHealth has also provided funding, e.g. to the Lao People’s Democratic Republic, for capacity-building on health promotion. Since 2011, ThaiHealth has served as the secretariat for the International Network for Health Promotion Foundation and provided in-kind support for its activities.
4.2 Monitoring and reporting system
ThaiHealth finances many short- and long-term programmes and relies on strategic partner- ships to initiate, design and implement its programmes to meet its objectives; it also has a project monitoring and reporting system to ensure that projects are progressing in accordance with their objectives and the time-bound deliverables. As mentioned above, 14 master plans are funded, with various programmes, each of which is administered by a “plan administering committee” comprising 7–15 external expert representatives of Government, NGOs, academic and other interest groups, including two Board members. They manage and administer the master plans, oversee the progress of projects and appoint a programme manager for each plan. ThaiHealth also funds an internal plan manager to oversee and monitor each plan and external work plan managers to oversee the work of one or more plans.
Each program is supported through the implementation of a series of projects as the lowest- level operational unit by an external organization. ThaiHealth acts as a facilitator and does not actually implement projects. Monitoring is built into each project, and progress is self-assessed by the grantees who are required in the signed contract to submit a financial and progress report to ThaiHealth at the end of each phase. Once the report is approved, subsequent financial support is released for the next stage of project activities. If the work plan or budget streams change, the steering committee can approve only a 10% budget adjustment during the same phase. For large projects, the plan administrative committee establishes a steering committee to supervise and report back to the administrative committee. The frequency of supervision for each cycle varies but may be every 3–12 months. Currently, ThaiHealth can estimate the benefit of granting support on the basis of the real outputs and outcomes of each project. In addition, an in-depth evaluation is made. Internal evaluations are carried out for projects costing 10 million baht (USD 0.33 million) or more, in which a project manager is required to report to the plan administrative committee. For the projects costing more than 20 million baht (USD 0.67 million), an external evaluation is carried out by each section and reported to the plan administrative committee. ThaiHealth uses independent external evaluators or groups for each project or programme to provide advice and support. For projects on major risk factors, evaluators work closely with the plan administrative committee and the project manager from the outset.
- Conclusions
A decade after its establishment, ThaiHealth is still learning to strengthen its programmes to meet its mission and vision. As a new financial mechanism was used, with a dedicated tax, awareness about ThaiHealth’s philosophy, governance and operational structures is still lacking. The tobacco and alcohol industries try to undermine the credibility of research findings and health promotion campaigns launched by ThaiHealth. Furthermore, the health promotion professionals and staff still have insufficient capability for health promotion and operational aspects, and their capacity must be strengthened continually. Inevitably, ThaiHealth sometimes encounters weak political support from the nine board members, most of whom are high-ranking officials in ministries that may have some political influence and also faces opposition from certain industries and businesses with vested interests. Despite these challenges, ThaiHealth continues to expand its scope of interest to respond to emerging health problems across Thailand with effective policies and programmes.
References
[1] Siwaraksa P. The birth of ThaiHealth Fund. Bangkok: Thai Health Promotion Foundation; 2002.
[2] Health Promotion Foundation Act, BE 2544 (2001). Bangkok: Government of Thailand; 2001.
[3] Caroll A, Wood L, Tantives S. Many things to many people: a review of ThaiHealth (2001–2006). Bangkok: World Health Organization and Thai Health Promotion Foundation; 2007.
[4] Galbally R, Fidler A, Chowdhury M, Tang KC, Good S, Tantivess S. Ten-year review of ThaiHealth Promotion Foundation (Nov 2001–Nov 2011). Bangkok: Thai Health Promotion Foundation; 2012.
[5] Vathesatogkit P, Tan YL, Ritthiphakdee B. Health Promotion Fund: sustainable financing and governance. Bangkok: Thai Health Promotion Foundation; 2013.
[6] Raungarreerat K. Overview of ThaiHealth. Presented during study the visit of the Viet Nam Tobacco Control Fund Team to ThaiHealth Foundation, Bangkok, 15–16 December 2014.
[7] Thai Health Promotion Foundation. Personal communication, 2015.
[8] Thailand’s budget in brief (fiscal years 2010, 2011, 2012, 2013 2014). Bangkok: Bureau of the Budget.
[9] Excise Department, Ministry of Finance, Thailand. Personal communication, 2012.
[10] Vathesatogkit P, Ritthiphakdee B. Thailand presentation on impact of tobacco tax policy. Presented at the workshop on the regional experience on tobacco tax, 5 July 2013, Halong, Quang Ninh, Vietnam.
[11] Levy DT, Benjakul S, Ross H, Ritthiphakdee B. The role of tobacco control policies in reducing smoking and deaths in a middle income nation: results from the Thailand SimSmoke simulation model. Tobacco Control 2008;17:53–59.
[12] Adulyanon S. Funding health promotion and disease prevention programmes: an innovative financing experience from Thailand. WHO South-East Asia J Public Health 2012;1:201–207.
[13] Social return on investment (SROI): selected cases from Thai Health Promotion Foundation. Bangkok: Thai Health Promotion Foundation; 2014.
[14] Raungarreerat K. ThaiHealth’s strategic plan and partners. Presented during study visit of Vietnam Tobacco Control Fund Team to ThaiHealth Foundation, Bangkok, 15–16 December 2014.
Related report
World Health Organization. (2016). Earmarked tobacco taxes: lessons learnt from nine countries. Geneva, World Health Organization.